
A few years back, I was at a cadaver workshop feeling pretty certain I was on the ‘right’ side of a surgical debate. Someone asked me why surgeons can’t get along when it comes to fixation versus non-fixation in minimally invasive surgery—it struck a chord. Why are we still fighting over screws and techniques when patients just want to walk without pain? Today, I’m pulling back the curtain on what I’ve learned, the data that changed my mind, and why I think it’s time for a new chapter in surgical education. (Spoiler: This isn’t a Yankees vs. Red Sox rivalry—at least, it shouldn’t be.)
1. Tribalism in Surgery: Why Do We Draw Lines in the Sand?
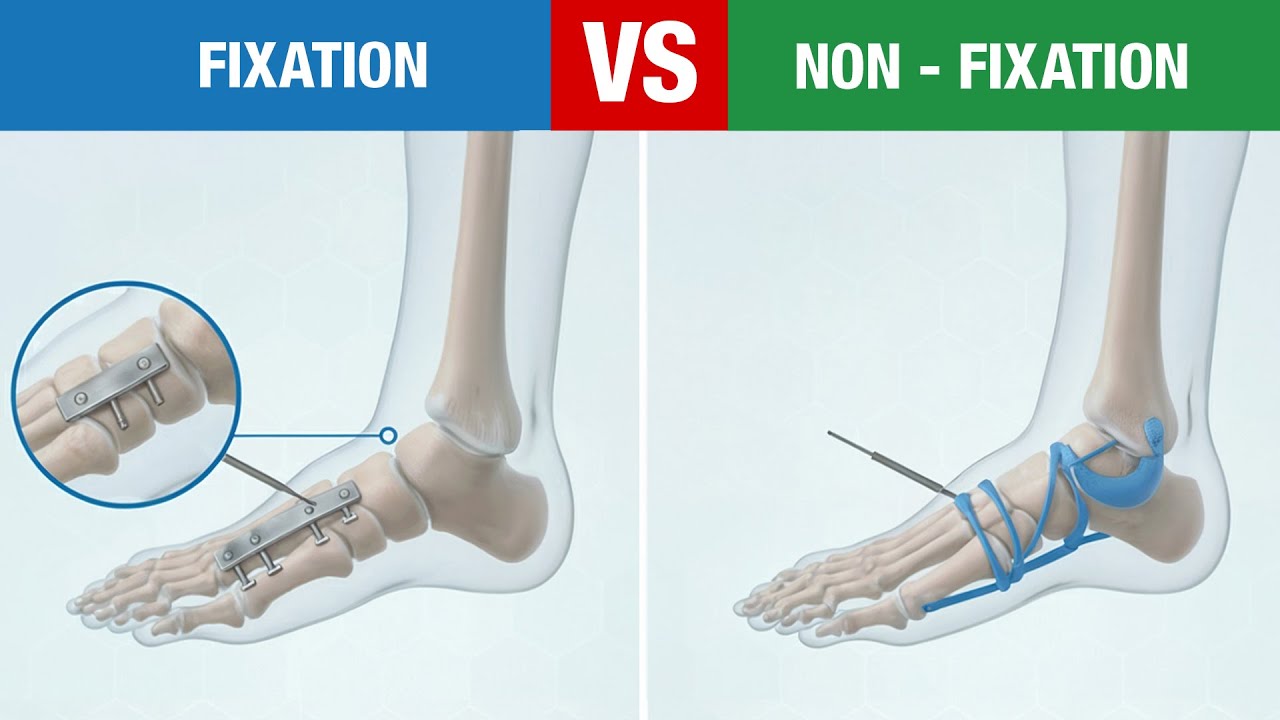
If you’ve spent any time in the world of Minimally Invasive Surgery (MIS), you know the Fixation Non-Fixation Debate is alive and well. Sometimes, it feels less like a scientific discussion and more like a heated sports rivalry—think Yankees versus Red Sox, but with scalpels and sutures. I see it every day, both online and in the operating room: surgeons drawing hard lines in the sand, fiercely defending their preferred techniques.
I’ll be honest—for years, I was firmly “team non-fixation.” I loved my non-fixation techniques: Reverdine-Isham, Modified Wilson, Reverse Austin, and others. These procedures felt elegant and effective when performed correctly. I was skeptical, even dismissive, of fixation-based MIS. It wasn’t just about the data; it was about identity and comfort zone.
But a question from an attendee at a recent MIS cadaver workshop made me pause: “Why is there so much fighting online about fixation versus non-fixation? Why can’t surgeons just get along?” It struck me how deeply this tribalism runs. We often see other philosophies as “foreign” or even risky, simply because we haven’t been exposed to them.
The real turning point for me was exposure and education.
The more I taught, the more I learned. The more surgeons I met from different backgrounds, the more I realized we are all trying to achieve the same thing—pain-free, happy patients.
Meeting colleagues with different training and surgeon experience opened my eyes to the strengths and limitations of both approaches. It became clear that our “tribal warfare” is often rooted in limited exposure, not evidence.
Surgeon experience, patient selection, and the training environment all shape our opinions. The ongoing Fixation Non-Fixation Debate in the surgical community isn’t just about technique; it’s about identity, tradition, and sometimes fear of the unknown. Yet, as research and collaboration continue, we’re reminded that there’s more than one path to excellent patient outcomes in Minimally Invasive Surgery.
2. Fact-Checking the Fixation vs. Non-Fixation Debate: Beyond Dogma
Let’s get real: whether you’re in the Fixation or Non-Fixation Group, we’re all aiming for the same outcome—pain-free, happy patients who recover quickly and avoid complications. But the debate between mesh fixation and non-fixation in minimally invasive surgery (MIS) often gets bogged down in dogma rather than data. So, let’s look at what the research actually says.
First, non-fixation is already widely accepted in several procedures. For example, DMMO for metatarsalgia and hammertoe corrections are routinely performed without fixation. Fifth metatarsal osteotomies? Also commonly done without hardware. Yet, when it comes to first ray non-fixation, many surgeons get nervous—and I get it. The first ray bears more load and is critical for foot function, so the stakes feel higher.
But here’s what changed my mind: a 2025 systematic review of 22 studies comparing fixation and non-fixation MIS found that both approaches led to faster recovery, lower complication rates, and higher patient satisfaction than traditional open reduction internal fixation. Notably, operative time was shorter in the non-fixation group compared to mesh fixation groups, and systemic review outcomes showed no significant difference in hospital stay between the two.
Worried about recurrence rate? Research in hernia repair and metatarsalgia procedures shows that non-fixation does not correlate with increased recurrence rates. In fact, a 2022 meta-analysis of over 1600 feet revealed that success wasn’t about fixation versus non-fixation—it was about surgeon experience and patient selection. Long-term data, like the 79-month Reverdine-Isham follow-up, confirms excellent results without fixation.
A masterfully done non-fixation procedure beats a poorly done fixation case. But equally, a well-executed MICA beats a sloppy Reverdine-Isham procedure.
So, what really matters? It’s not the technique itself, but:
- Surgeon training and comfort level
- Patient factors: bone quality, activity level, expectations
- Deformity characteristics and associated conditions
- Postoperative pain management and aftercare protocols
Ultimately, both fixation and non-fixation MIS can deliver outstanding results when matched to the right patient and performed with skill. The evidence urges us to move beyond rivalry and focus on what works best for each individual.
3. Choosing the Right Tool: How Training and Flexibility Shape MIS Outcomes
In Minimally Invasive Surgery, the difference between a good and a great outcome often comes down to one thing: choosing the right tool for the right patient. It’s not about fixation versus non-fixation as rival camps—it’s about matching the procedure to the patient’s unique needs. Patient outcomes rise when surgeons pick procedures based on patient specifics, not dogma.
As I’ve seen in countless MIS education workshops, surgeon experience and patient selection are critical. Factors like bone quality, activity level, the severity and characteristics of the deformity, and patient expectations all play a role. For example, a high-activity patient with robust bone may do well with one approach, while a patient with osteoporosis or complex deformity may need another. Surgeon comfort and training also matter—no technique is truly safe or effective in hands that aren’t well-trained.
Unfortunately, many surgeons only learn one philosophy during training. I often see heated debates online, with statements like “there’s no evidence for non-fixation” or “that’s not evidence-based.” But in reality, the evidence is there—it’s published and peer-reviewed. The real issue is lack of exposure, not lack of data. If you’ve only seen one way, everything else feels foreign, maybe even risky. That’s not malicious; it’s just limited experience.
That’s why I’m passionate about building MIS education workshops that break down these silos. My vision is simple: bring together the best experts in both fixation and non-fixation, so every surgeon gets exposed to every tool in the toolbox. As I always say:
That’s not biased. That’s complete education. So you get exposed to every tool in the toolbox, taught by the people who know each tool best.
Imagine a workshop where I teach foundational non-fixation techniques, a MICA expert demonstrates their approach, and a SERI specialist shares their pearls. Everyone learns from everyone. This collaborative model advances both fixation and non-fixation practices, improves patient outcomes, and fosters a stronger surgical community.
When surgeons see all philosophies side by side—taught at the highest level—they gain the flexibility to tailor procedures to each patient. That’s how we move beyond rivalry and focus on what matters most: patient outcomes and surgical excellence.
4. Wild Card: Patients Don’t Care About Our Rivalries—They Want Results
Here’s something we often forget in the heat of the Fixation Non-Fixation Debate in Minimally Invasive Surgery: while we’re busy arguing about screws versus no screws, our patients are just hoping someone can help them walk without pain. The truth is, patients aren’t invested in our philosophical debates—they care about recovery, mobility, and, above all, patient satisfaction.
While we’re arguing about screws versus no screws, our patients are just hoping someone can help them walk without pain.
Minimally Invasive Surgery has already proven itself by delivering higher patient satisfaction and better recovery rates compared to traditional open procedures. Whether you choose fixation or non-fixation, both approaches can deliver excellent results when performed with skill and attention to the patient’s unique needs. The real measure of success isn’t which technique we prefer, but whether our patients are able to return to their lives with less pain and more function.
As surgeons, it’s easy to get caught up in defending our favorite techniques. But let’s be honest—our patients don’t care about our rivalries. They care about outcomes. They want to know: Will I be able to walk without pain? Will I recover quickly? Will I be satisfied with my care? These are the questions that matter most.
That’s why I’m inviting you—my colleagues in the surgical community—to share your real-world experiences. Have you tried both fixation and non-fixation in Minimally Invasive Surgery? What have you learned? What factors guide your decision for each patient? Let’s move beyond opinions and focus on what truly helps our patients. Share your pearls in the comments, not your prejudices. The best insights will be featured in my next video, because I’m not just building workshops—I’m building bridges.
In the end, the fixation vs. non-fixation debate should never overshadow our shared goal: delivering the best possible results for our patients. Let’s keep the conversation constructive, collaborative, and always centered on patient satisfaction. That’s how we move forward—not just as surgeons, but as a community dedicated to better care.
TL;DR: Both fixation and non-fixation approaches in minimally invasive surgery can produce excellent results. The real secret? Skill, evidence, and open-minded collaboration—not rivalry.